I wear a lot of hats in my job. Though I’m a physician who specializes in the practice of anesthesiology, I don’t spend all day every day at the head of an operating room table.
Many days I spend in an administrative leadership role or conducting research studies. These functions support the best interests of my patients as well as the science and practice of anesthesiology. On my “clinical” days that I spend in hands-on patient care, I provide anesthesia for patients who undergo surgery and other invasive procedures. I also treat acute pain as a consultant. Some of my colleagues in anesthesiology specialize in chronic pain or critical care medicine.
As a medical student, I had a hard time at first understanding what the physician anesthesiologist does. I saw monitors, complicated equipment, and technical procedures that involved a lot of needles. Thankfully, I worked with resident and attending anesthesiologists who inspired me to pursue this specialty.
Anesthesiology is a unique field within medicine. It is at the same time incredibly cerebral and extremely physical. For example, the physician anesthesiologist must be ready to diagnose heart or lung problems that may complicate the patient’s surgery, and decide which medications are appropriate.
Before administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.
I am always aware of the trust that patients and their families give me, a total stranger, and I work hard to earn that trust throughout the perioperative period. The job of the physician anesthesiologist is deeply personal. In the operating room, I care for the most vulnerable of patients—those who, while under anesthesia, cannot care for themselves.
– I constantly listen to the sounds of their hearts. – I breathe for them when they are unable. – I keep them warm in the cold operating room. – I provide the fluids that their bodies need. – I pad their arms and legs and other pressure points. – I watch the operation step by step, anticipating and responding. – I learn from their bodies’ response to anesthesia to give the right amount. – I prevent and relieve their pain. – I protect them from dangers of which they are unaware.
I have heard people, my colleagues included, compare physician anesthesiologists to pilots. No one claps when the plane lands, just as no one expects any less than a perfect uncomplicated anesthetic every time. We physician anesthesiologists draw great personal satisfaction from doing what we do, and from providing a unique type of personalized medicine. Our patients and their families depend on us to be at our best, always.
We have all heard the “doom and gloom” statistics about rising health care spending, and maybe even some of them have begun to sink in since the roll-out of the Affordable Care Act.
For many reasons, the federal government is working to curb health care expenditures, but many of the processes currently attributed to “Obamacare” have been in the works for a long time. As an example, the Medicare Modernization Act of 2003 introduced the Inpatient Prospective Payment System; this system encouraged participating hospitals to voluntarily report performance data to avoid payment reductions. The Deficit Reduction Act of 2005 went further by mandating the development of what we now know as pay-for-performance or value-based purchasing (used interchangeably).
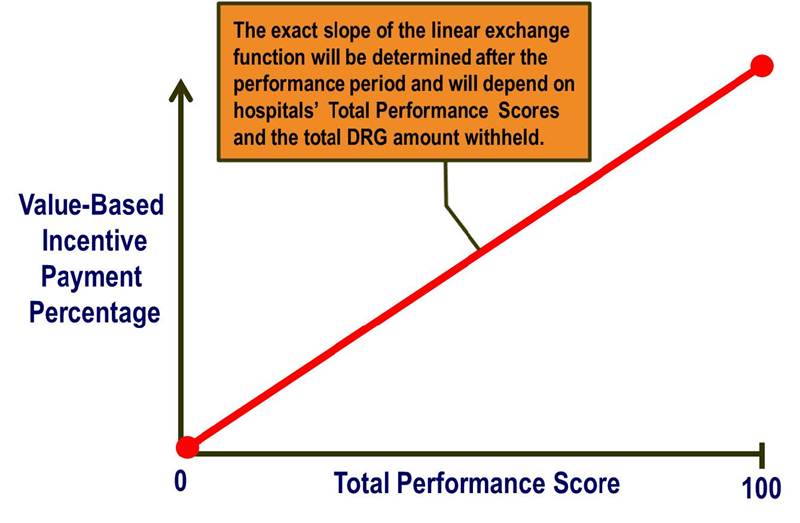
What does this mean? Value-based purchasing in health care is supposed to reward better value, patient outcomes, and innovations – instead of just volume of services (read more). It is funded by participating institutions based on withholding a set percentage (1.25% currently) of their estimated annual Diagnosis-Related Group (DRG) payments from Center for Medicare and Medicaid Services (CMS). The percentage is increasing every year and will be 2% by 2017.
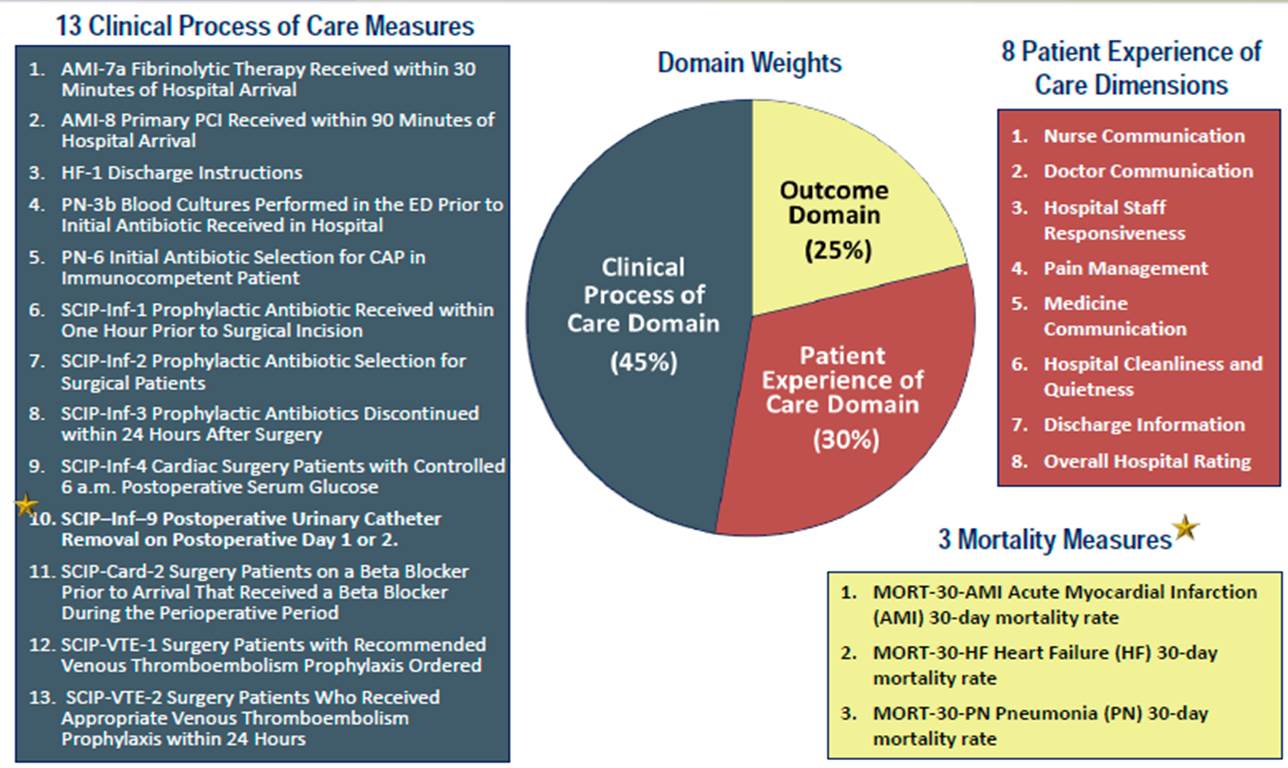
For FY2014, the elements of value-based purchasing have been updated to include the Clinical Process of Care Domain, Patient Experience of Care Domain, and a new Outcomes Domain. The amount that each of these domains contributes to the eventual DRG payment return at the end of the year is 45%, 30%, and 25%, respectively. Scores in each domain are calculated based on an institution’s improvement compared to its own historical performance and a comparison against national benchmarks (read more).
How do we as anesthesiologists address the need for acute pain medicine physicians and have a positive impact on the patient experience? We can take the lead in developing multimodal perioperative pain management protocols (1). For total joint arthroplasty, many of these protocols emphasize opioid-sparing regional anesthesia techniques such as peripheral nerve blocks (PNB) and perineural catheters. These techniques decrease patients’ reliance on opioids for postoperative pain management and are also associated with fewer opioid-related side effects, better sleep, and higher satisfaction (2). In addition, greater selectivity in the PNB technique included in a multimodal protocol may even lead to greater functional achievements for total knee arthroplasty (TKA) patients which generates additional value (3). For more information about TKA perioperative pain management and improving rehabilitation outcomes, please see my previous post “Regional Anesthesia & Rehabilitation Outcomes after Knee Replacement.”
Anesthesiologists can also add value through cost savings for the hospital. More effective pain management can prevent inadvertent admissions or readmissions due to pain. In addition, an effective multimodal analgesic protocol can directly or indirectly prevent hospital-acquired conditions (HACs). HACs are considered by CMS to be “never events” and supposedly preventable (4); hospitals reporting HACs as secondary diagnoses are not entitled to CMS payments for related care. Examples of HACs include: urinary and vascular catheter-related infections, surgical site infections, DVT/PE, pressure ulcers, and inpatient falls leading to injury.
There remains substantial controversy related to the potential association between regional anesthesia and inpatient falls (5, 6). We do know that falls, when they occur, are associated with worse outcomes for patients and higher resource utilization (7) and that falls may occur in lower extremity joint replacement patients with or without PNB (8). For these reasons, these patients should always be treated as high fall risk, and anesthesiologists can take the lead in developing fall prevention education and fall reduction programs to keep them safe.
In summary, pay for performance in perioperative pain management is already here. The HCAHPS survey assesses the Patient Experience Domain and can be heavily influenced by the effectiveness of pain management. There are clear opportunities for anesthesiologists to take an active role in adding value and minimizing risks for surgical patients in the perioperative period.
References:
Hebl JR, Kopp SL, Ali MH, Horlocker TT, Dilger JA, Lennon RL, Williams BA, Hanssen AD, Pagnano MW. A comprehensive anesthesia protocol that emphasizes peripheral nerve blockade for total knee and total hip arthroplasty. J Bone Joint Surg Am 2005;87 Suppl 2:63-70.
Ilfeld BM. Continuous peripheral nerve blocks: a review of the published evidence. Anesth Analg 2011;113:904-25.
Mudumbai SC, Kim TE, Howard SK, Workman JJ, Giori N, Woolson S, Ganaway T, King R, Mariano ER. Continuous Adductor Canal Blocks Are Superior to Continuous Femoral Nerve Blocks in Promoting Early Ambulation After TKA. Clinical orthopaedics and related research 2014;472:1377-83.
Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg 2010;111:1552-4.
Memtsoudis SG, Danninger T, Rasul R, Poeran J, Gerner P, Stundner O, Mariano ER, Mazumdar M. Inpatient falls after total knee arthroplasty: the role of anesthesia type and peripheral nerve blocks. Anesthesiology 2014;120:551-63.
Memtsoudis SG, Dy CJ, Ma Y, Chiu YL, Della Valle AG, Mazumdar M. In-hospital patient falls after total joint arthroplasty: incidence, demographics, and risk factors in the United States. The Journal of arthroplasty 2012;27:823-8 e1.
Johnson RL, Kopp SL, Hebl JR, Erwin PJ, Mantilla CB. Falls and major orthopaedic surgery with peripheral nerve blockade: a systematic review and meta-analysis. Br J Anaesth 2013;110:518-28.
The concept of preoperative preparation for patients scheduled for surgery requiring anesthesia is not a new one. In fact, the idea goes back to Dr. Albert Lee’s description in 1949 (1, 2). Dr. Lee had observed in his day that patients commonly presented for surgery in various states of poor health; it seemed to make more sense to see these patients before surgery to identify areas of concern early and optimize patients’ conditions they went under the knife.
The model of a stand-alone preoperative evaluation clinic, often run by anesthesiology staff, with a “one stop shop” model for patients’ interviews and examinations, testing, education, and referrals really did not take off until the 1990s (3). This patient-centered care model was intended to improve efficiency by decreasing the run-around that many patients encountered, but it also saved money for the institution by reducing the ordering of unnecessary tests (4) and decreasing day-of-surgery cancellations (4, 5).
Current State
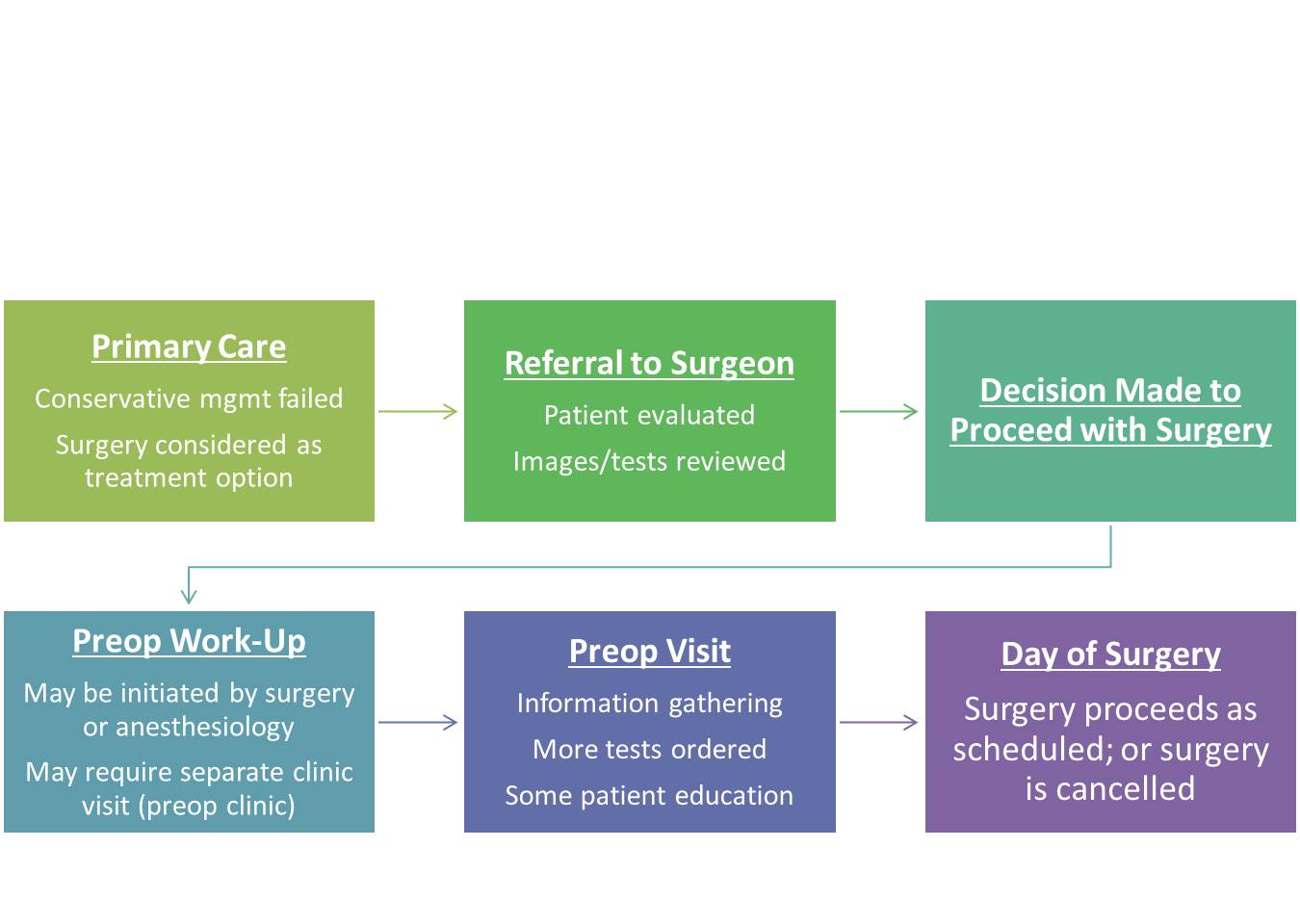
In the present state (assuming an ACO or HMO model), patients are referred to the surgeon by the primary care physician for evaluation of a problem that may be amenable to surgical correction. If the surgeon deems the patient a surgical candidate, the patient may receive a scheduled date for surgery and then may be referred to the anesthesiology preoperative evaluation clinic (“preop clinic”) for further work-up. During this encounter, the provider in the preop clinic may request a variety of tests based on the planned surgery and the patient’s comorbid conditions in order to make appropriate recommendations regarding perioperative management to minimize risks. The American Society of Anesthesiologists (ASA) has published a recent (2012) practice advisory for preanesthesia evaluation to guide this process.
Unfortunately, after nearly 2 decades of employing this model, day of surgery cancellations still occur at various rates around the world. Some of the reasons are related to factors that preop clinics were meant to avoid: inadequate preoperative work-up or change in medical condition (6). Other reasons are patient-driven: patients’ not showing up (7) or patients’ changing their minds about having surgery (8). Although not all of these issues are easily solved, it does make me wonder–perhaps it is time for us to rethink the process of preparing patients for surgery.
In our current state, a patient may hypothetically be scheduled for surgery in 8 weeks, a date agreed upon by the patient and surgeon based on available dates. Even if a preop clinic visit takes place the same day as the surgery clinic visit, this only allows 2 months to optimize a patient’s chronic medical conditions (e.g., hypertension, diabetes, coronary artery disease) that took years to develop. Imagine if the timeline was even shorter, like 3 weeks. Add to this time pressure the tremendous physiologic stress that surgery and the subsequent rehabilitation put on the body, and it is not difficult to see why patients can still be cancelled on the day of surgery when they present with abnormal vital signs or test results, making the risks seem too high. We would not expect ourselves to run a marathon without adequate training and preparation on short notice–why would we do this to our patients having elective surgery?
Future State
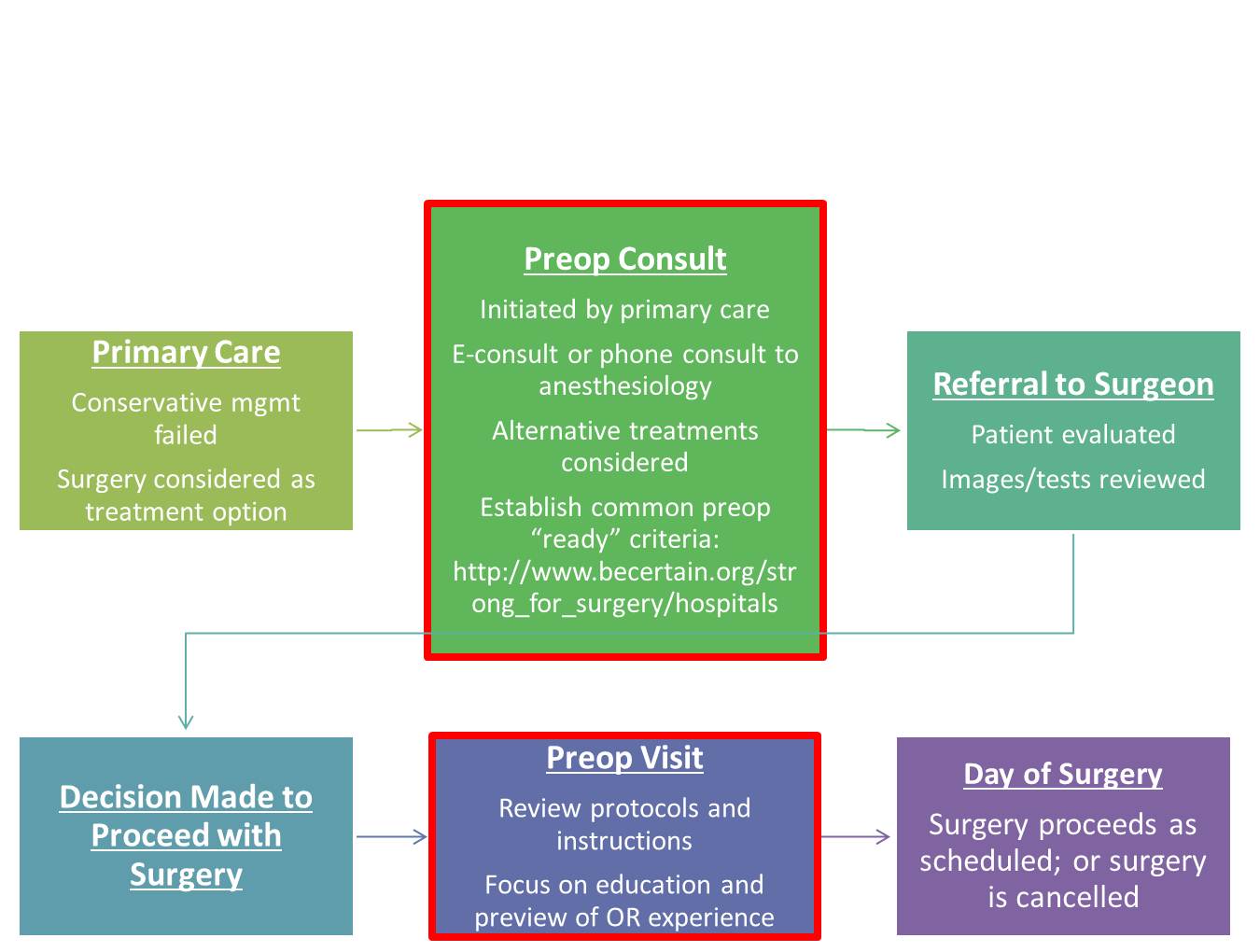
How can we improve preoperative preparation? I think it still starts with the primary care physician. With advances in technology such as telemedicine and e-consults (or low-tech phone calls), we have ways to create a direct interface between primary care physicians and anesthesiologists to discuss advanced preparation of patients who may undergo elective surgical procedures.
This coordinated care model is consistent with ASA’s Perioperative Surgical Home. Early consultation may involve assessment of a patient’s risks and benefits from the procedure, consideration of alternative treatments, and development of a plan to optimize the patient’s comorbid conditions, medication management, and nutrition. Strong for Surgery is a program that provides patients and clinicians useful checklists based on best-available evidence to guide early preoperative preparation related to smoking cessation, nutrition, glycemic control, and medication management. For elective surgery, the decision when to refer the patient to a surgeon can be made jointly by the primary care physician and anesthesiologist. Prior to surgery, the preop clinic visit should still take place, but the focus no longer needs to be on information-gathering and ordering a battery of tests; rather, the goals should be to review pertinent instructions, preview the perioperative experience for patients, and address any logistical or scheduling issues raised by patients to prevent their not showing up or changing their minds at the last minute. Let’s get started.
Chronic pain can be palliated, but “acute” pain (new onset, often with an identifiable cause) must be stamped out. This requires a systems-based approach led by physicians dedicated to understanding acute pain pathophysiology and investigating new ways to treat it. The solution is definitely not giving more and more opioids.
As our understanding of pain mechanisms has evolved, select physicians have developed a special focus on pain in the acute injury/illness and perioperative settings that has led to the rapid advancement of systemic and site-specific interventions to effectively manage this type of pain. Acute pain medicine involves the routine use of multiple modalities concurrently (i.e., multimodal analgesia) in the in-hospital setting to reduce the intensity of acute pain and minimize the development of debilitating persistent pain, a problem that can result from even common surgical procedures or trauma. Unfortunately, the need for specialists in acute pain medicine is increasing.
In December of 2013, I submitted a 161 page letter to the Accreditation Council for Graduate Medical Education (ACGME) requesting that regional anesthesiology and acute pain medicine be considered for fellowship accreditation with the help of my fellowship director colleagues. The Board of Directors of the ACGME informed me this past fall (2014) that they have approved our fellowship to be the next accredited subspecialty within anesthesiology.
Wait – don’t we already have a fellowship program in pain medicine? Yes we do, and this one year post-residency program does include the “Acute Pain Inpatient Experience.” However, this requirement may be satisfied by documented involvement with a minimum of only 50 new patients and is not the primary emphasis of fellowship training in the specialty. Pain medicine is a board-certified subspecialty of anesthesiology, physical medicine and rehabilitation, and psychiatry and neurology; graduates from any of these residency programs can apply to the one year program. In a recent survey study of practicing pain physicians in the United States with added qualification in pain management according to the American Board of Medical Specialties (ABMS), the great majority (83.7%) of respondents defined their practices as following “chronic pain patients longitudinally” (1).
There is clearly room and a need for a subspecialty training program in acute pain medicine that can focus on improving the in-hospital pain experience. Such a program should advance, in a positive and value-added fashion, the present continuum of training in pain medicine.
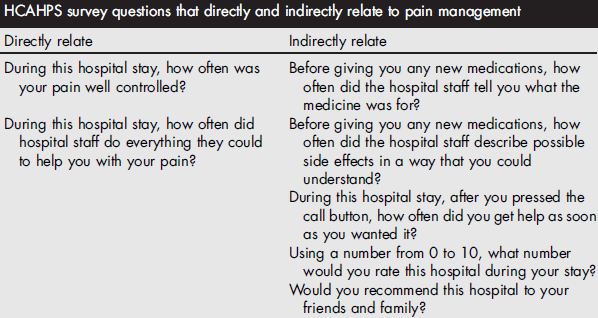
The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey is administered to a random sample of patients who have received inpatient care and receive government insurance through Center for Medicare and Medicaid Services (CMS). The survey consists of 32 questions and is intended to assess the “patient experience of care” domain in the value-based purchasing program. A hospital’s survey scores are publicly disclosed and make up 30% of the formula used to determine how much of its diagnosis-related group payment withholding will be paid by CMS at the end of each year. Of the 32 questions, 7 directly or indirectly relate to in-hospital pain management.
Why should acute pain medicine be a subspecialty of anesthesiology? Anesthesiology is a hospital-based medical specialty, and anesthesiologists are physicians who focus on the prevention and treatment of pain for their patients who undergo surgery, suffer trauma, or present for childbirth on a daily basis. For more details on the role of the anesthesiologist, please see “Physicians specializing in the patient experience.” Further, history supports the evolution of acute pain medicine through anesthesiology. The concept of an anesthesiology-led acute pain management service was described first in 1988 (2), but arguably the techniques employed in modern acute pain medicine and regional anesthesiology date back to Gaston Labat’s publication of Regional Anesthesia: its Technic and Clinical Application in 1922, with advancement and refinement of this subspecialty in the 1960s and 1970s (3-7).
By the time they complete the core residency in anesthesiology today, not all trainees have gained sufficient clinical experience to provide optimal care for the complete spectrum of issues experienced by patients suffering from acutely painful conditions, including the ability to reliably provide advanced interventional techniques proven to be effective in managing pain in the acute setting (8-12). We need physician leaders who can run acute pain medicine teams and design systems to provide individualized, comprehensive, and timely pain management for both medical and surgical patients in the hospital, expeditiously managing requests for assistance when pain intensity levels exceed those set forth in quality standards, or to prevent pain intensity from reaching such levels. The mission statement for the Acute Pain Medicine Special Interest Group within the American Academy of Pain Medicine provides additional justification.
In a survey of fellowship graduates and academic chairs published in 2005, 61 of 132 of academic chairs responded (46%), noting that future staffing models for their department will likely include an average of 2 additional faculty trained in regional anesthesiology and acute pain medicine (13).
Currently, there are over 60 institutions in the United States and Canada that list themselves as having non-accredited fellowship training programs focused on regional anesthesiology and acute pain medicine on the ASRA website. Since 2002, the group of regional anesthesiology and acute pain medicine fellowship directors has been meeting twice yearly at the ASRA Spring Annual Meeting and ASA Annual Meeting which takes place in the fall. Despite not being an ACGME-accredited fellowship, this group, recognizing the lack of formalized training guidelines, voluntarily began to develop such guidelines as the foundation for subspecialty fellowship training in existing and future programs. These guidelines were originally published in Regional Anesthesia and Pain Medicine in 2005 (14), then were subsequently reviewed, revised, and published as the 2nd edition in 2011 (15), and have been recently updated again (16).
As with other subspecialties, acute pain medicine has emerged due to the need for trained specialists—in this case, those who understand the complicated, multi-faceted disease processes of acute pain, and its potential continuity with chronic pain, and can apply appropriate medical and interventional treatment in a timely fashion. The fellowship-trained regional anesthesiologist and acute pain medicine specialist must be capable of collaborating with other healthcare providers in anesthesiology, surgery, medicine, nursing, pharmacy, physical therapy, and more to establish multidisciplinary programs that add value and improve patient care in the hospital setting and beyond.
REFERENCES
Breuer B, Pappagallo M, Tai JY, Portenoy RK: U.S. board-certified pain physician practices: uniformity and census data of their locations. J Pain 2007; 8: 244-50
Ready LB, Oden R, Chadwick HS, Benedetti C, Rooke GA, Caplan R, Wild LM: Development of an anesthesiology-based postoperative pain management service. Anesthesiology 1988; 68: 100-6
Winnie AP, Ramamurthy S, Durrani Z: The inguinal paravascular technic of lumbar plexus anesthesia: the “3-in-1 block”. Anesth Analg 1973; 52: 989-96
Winnie AP, Collins VJ: The Subclavian Perivascular Technique of Brachial Plexus Anesthesia. Anesthesiology 1964; 25: 353-63
Raj PP, Parks RI, Watson TD, Jenkins MT: A new single-position supine approach to sciatic-femoral nerve block. Anesth Analg 1975; 54: 489-93
Raj PP, Rosenblatt R, Miller J, Katz RL, Carden E: Dynamics of local-anesthetic compounds in regional anesthesia. Anesth Analg 1977; 56: 110-7
Buvanendran A, Kroin JS: Multimodal analgesia for controlling acute postoperative pain. Curr Opin Anaesthesiol 2009; 22: 588-93
Hebl JR, Dilger JA, Byer DE, Kopp SL, Stevens SR, Pagnano MW, Hanssen AD, Horlocker TT: A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med 2008; 33: 510-7
Jin F, Chung F: Multimodal analgesia for postoperative pain control. J Clin Anesth 2001; 13: 524-39
Kehlet H, Dahl JB: The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg 1993; 77: 1048-56
Young A, Buvanendran A: Recent advances in multimodal analgesia. Anesthesiol Clin 2012; 30: 91-100
Neal JM, Kopacz DJ, Liguori GA, Beckman JD, Hargett MJ: The training and careers of regional anesthesia fellows–1983-2002. Reg Anesth Pain Med 2005; 30: 226-32
Among Medicare beneficiaries in the United States, the number of primary total knee arthroplasty (TKA) procedures from 1991 to 2010 increased by 161.5% (1). Postoperative pain remains one of patients’ top concerns when undergoing elective surgery (2) and can limit patients’ functional ability in the early postoperative period (3). Providing effective perioperative pain control has potential longer-term implications since early rehabilitation may lead to improvements in functional outcomes later on (4). With the ability to select specific targets for local anesthetic injection and infusion, regional anesthesia techniques, neuraxial and peripheral, are commonly included in the perioperative analgesic protocol for joint arthroplasty patients (5-11). While the data supporting the analgesic efficacy of regional anesthesia techniques in this setting are strongly positive, studies attempting to attribute functional outcome benefits to regional anesthesia demonstrate mixed results.
The main challenge in assessing functional outcomes following joint replacement is the selection of outcomes; these can be divided into performance-based outcomes and self-reported outcomes (12, 13). Performance-based outcomes are measurable and arguably more objective, although often subject to effort. Examples of these outcomes and their units of measure include joint range of motion in degrees (e.g., flexion, extension, rotation); timed walking tests in meters (e.g., 6 minute walking test [6MWT], 2 minute walking test [2MWT]); muscle strength in units of force using a dynamometer (e.g., maximum voluntary isometric contraction [MVIC]); and timed up-and-go (TUG) in minutes (12, 13). Self-reported outcomes are typically survey-based; examples include the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC), Knee Society Score, and Lower Extremity Functional Scale (12, 13). Since patient perception of successful rehabilitation is an important factor, self-reported outcomes should be reported with performance-based outcomes (12). Another important challenge when measuring and comparing functional outcomes is that clinical pathways for joint arthroplasty that integrate pain management (including regional analgesia), physical therapy, nursing, and surgical care are often specific to individual institutions, and institutions may vary with respect to rehabilitation goals and the timeline to achieve them.
Epidural Analgesia
Epidural analgesia has been used for perioperative pain management in joint replacement patients since at least the 1980s (14, 15). In 1987, Raj and colleagues compared postoperative systemic opioid analgesia to continuous epidural analgesia (bupivacaine 0.25% at 6-15 ml/hr) for TKA patients in a prospective non-randomized study (14). Although pain scores were lower in the epidural group, not surprisingly a high proportion of these patients experienced complete motor block of the lower extremities; although the authors mention “rigorous passive exercises,” specific rehabilitation outcomes were not reported (14). Later studies have reported functional benefits associated with continuous epidural analgesia, such as shorter time to achieve ambulation distance and range of motion goals, when compared to parenteral opioids alone (16). At institutions where continuous epidural analgesia is currently employed as part of a multimodal analgesic protocol, very low doses of local anesthetic (e.g., 0.06% bupivacaine) in combination with opioid are used in order to minimize motor block (17).
Peripheral Nerve Blocks
The innervation of the knee is complex and involves contributions from both the lumbar and sacral plexuses. While epidural analgesia is effective, it is also associated with clinically-significant side effects (e.g., nausea/vomiting and motor block of the non-operative limb) (5, 18) and the potential for neuraxial hematoma in patients on pharmacologic thromboprophylaxis (19). Thus, peripheral nerve block options, either single-injection or continuous infusions, have been explored for postoperative pain management.
Two early studies by Capdevila (6) and Singelyn (20) have shown continuous femoral nerve block (FNB) to provide comparable analgesia and physical therapy outcome achievement with fewer side effects when compared to epidural analgesia. Both of these studies also demonstrated shorter hospital length of stay for the regional anesthesia groups compared to an opioid-only group (6, 20), but hospitalization duration for these studies was, on average, greater than what has been reported in other studies (21). Triple-masked, placebo-controlled randomized clinical trials have shown that CPNB can shorten the time to achieve discharge criteria, including 100 m ambulation distance, for TKA (10, 22) and total hip arthroplasty (THA) (9) patients, but actual hospital duration was similar in these studies.
One of the interesting findings from the Singelyn study was that regional anesthesia patients maintained a knee flexion advantage over the opioid-only group at 6 week follow-up (20); although this advantage did not remain at 3 months, this finding supported the potential for long-term functional improvement resulting from effective pain management and early rehabilitation in the immediate perioperative period (4). In a randomized comparison of continuous FNB to local infiltration analgesia (LIA) for TKA, the FNB group spent more time out of bed walking; at 6 weeks, the FNB group showed more improvement in performance-based (6MWT) and self-reported functional outcome assessments (23). In contrast, the one year follow-up studies of randomized clinical trial subjects (9, 10, 22) using self-reported outcome measures for functional status (WOMAC) did not show long-term improvement associated with regional anesthesia techniques (24-27).
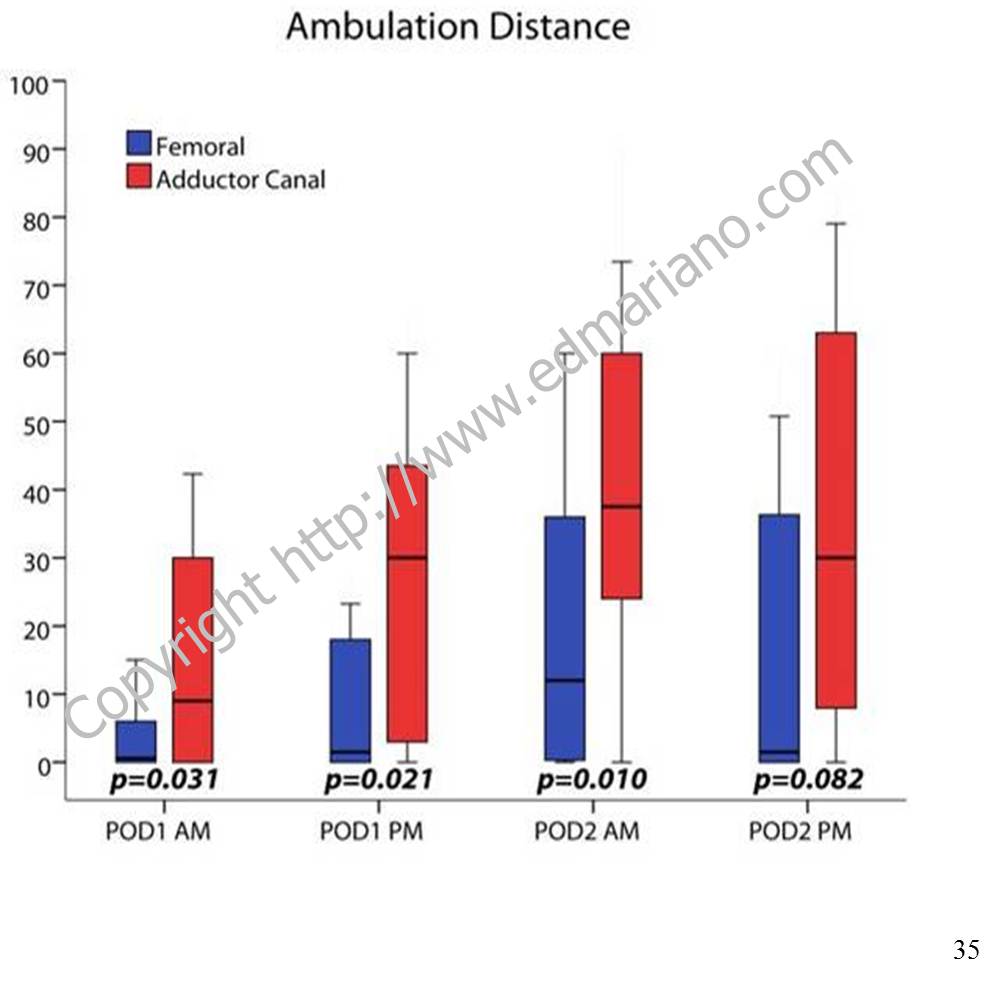
The rehabilitation outcome measured in the immediate postoperative period that correlates best with long-term functional improvement is not yet established. Ambulation distance is often measured by physical therapists and included in discharge criteria (9, 10, 22). For institutions that emphasize ambulation in their clinical pathway for lower extremity joint arthroplasty, a major concern raised with regard to FNBs is the potential association with increased fall risk (28, 29) although a recent large database study disputes this finding. In-hospital falls can lead to prolonged hospital stays with higher costs and are associated with more frequent postoperative complications, including serious organ system dysfunction and death (30). With currently-available local anesthetic solutions and typical doses, perineural infusion does produce clinically-significant quadriceps weakness when administered near the femoral nerve or lumbar plexus (31, 32). Since the local anesthetics themselves cannot select sensory over motor nerves( 33), anesthesiologists have started exploring alternate nerve block locations to minimize the risk of motor block and maximize patient rehabilitation.
From Workman JJ, et al. Presented at 2013 ASRA Spring Annual Meeting
For TKA, a more distal nerve block location in the adductor canal can provide effective analgesia postoperatively (34) and has been shown to better preserve quadriceps strength compared to a FNB in both volunteers (35) and clinical patients (11). Regional analgesic techniques are only one part of the overall pain management plan. While they are often included in multimodal analgesic protocols along with non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and low-dose opioids (36), there is a growing body of evidence to support the adductor canal block as the regional analgesic technique of choice for promoting postoperative ambulation within a clinical pathway (37, 38).
For patient information with answers to frequently-asked questions about regional anesthesia, please see “Regional Anesthesia FAQs.”
References
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. Sep 26 2012;308(12):1227-1236.
Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. Sep 1999;89(3):652-658.
Holm B, Kristensen MT, Myhrmann L, et al. The role of pain for early rehabilitation in fast track total knee arthroplasty. Disability and rehabilitation. 2010;32(4):300-306.
Munin MC, Rudy TE, Glynn NW, Crossett LS, Rubash HE. Early inpatient rehabilitation after elective hip and knee arthroplasty. JAMA. Mar 18 1998;279(11):847-852.
Barrington MJ, Olive D, Low K, Scott DA, Brittain J, Choong P. Continuous femoral nerve blockade or epidural analgesia after total knee replacement: a prospective randomized controlled trial. Anesth Analg. Dec 2005;101(6):1824-1829.
Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. Jul 1999;91(1):8-15.
Chelly JE, Greger J, Gebhard R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty. Jun 2001;16(4):436-445.
Hebl JR, Dilger JA, Byer DE, et al. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. Nov-Dec 2008;33(6):510-517.
Ilfeld BM, Ball ST, Gearen PF, et al. Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial. Anesthesiology. Sep 2008;109(3):491-501.
Ilfeld BM, Le LT, Meyer RS, et al. Ambulatory continuous femoral nerve blocks decrease time to discharge readiness after tricompartment total knee arthroplasty: a randomized, triple-masked, placebo-controlled study. Anesthesiology. Apr 2008;108(4):703-713.
Jaeger P, Zaric D, Fomsgaard JS, et al. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med. Nov-Dec 2013;38(6):526-532.
Choi S, Trang A, McCartney CJ. Reporting functional outcome after knee arthroplasty and regional anesthesia: a methodological primer. Reg Anesth Pain Med. Jul-Aug 2013;38(4):340-349.
Bernucci F, Carli F. Functional outcome after major orthopedic surgery: the role of regional anesthesia redefined. Curr Opin Anaesthesiol. Oct 2012;25(5):621-628.
Raj PP, Knarr DC, Vigdorth E, et al. Comparison of continuous epidural infusion of a local anesthetic and administration of systemic narcotics in the management of pain after total knee replacement surgery. Anesth Analg. May 1987;66(5):401-406.
Pettine KA, Wedel DJ, Cabanela ME, Weeks JL. The use of epidural bupivacaine following total knee arthroplasty. Orthopaedic review. Aug 1989;18(8):894-901.
Mahoney OM, Noble PC, Davidson J, Tullos HS. The effect of continuous epidural analgesia on postoperative pain, rehabilitation, and duration of hospitalization in total knee arthroplasty. Clin Orthop Relat Res. Nov 1990(260):30-37.
YaDeau JT, Cahill JB, Zawadsky MW, et al. The effects of femoral nerve blockade in conjunction with epidural analgesia after total knee arthroplasty. Anesth Analg. Sep 2005;101(3):891-895, table of contents.
Zaric D, Boysen K, Christiansen C, Christiansen J, Stephensen S, Christensen B. A comparison of epidural analgesia with combined continuous femoral-sciatic nerve blocks after total knee replacement. Anesth Analg. Apr 2006;102(4):1240-1246.
Horlocker TT, Wedel DJ, Rowlingson JC, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. Jan-Feb 2010;35(1):64-101.
Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. Jul 1998;87(1):88-92.
Salinas FV, Liu SS, Mulroy MF. The effect of single-injection femoral nerve block versus continuous femoral nerve block after total knee arthroplasty on hospital length of stay and long-term functional recovery within an established clinical pathway. Anesth Analg. Apr 2006;102(4):1234-1239.
Ilfeld BM, Mariano ER, Girard PJ, et al. A multicenter, randomized, triple-masked, placebo-controlled trial of the effect of ambulatory continuous femoral nerve blocks on discharge-readiness following total knee arthroplasty in patients on general orthopaedic wards. Pain. Sep 2010;150(3):477-484.
Carli F, Clemente A, Asenjo JF, et al. Analgesia and functional outcome after total knee arthroplasty: periarticular infiltration vs continuous femoral nerve block. Br J Anaesth. Aug 2010;105(2):185-195.
Ilfeld BM, Shuster JJ, Theriaque DW, et al. Long-term pain, stiffness, and functional disability after total knee arthroplasty with and without an extended ambulatory continuous femoral nerve block: a prospective, 1-year follow-up of a multicenter, randomized, triple-masked, placebo-controlled trial. Reg Anesth Pain Med. Mar-Apr 2011;36(2):116-120.
Morin AM, Kratz CD, Eberhart LH, et al. Postoperative analgesia and functional recovery after total-knee replacement: comparison of a continuous posterior lumbar plexus (psoas compartment) block, a continuous femoral nerve block, and the combination of a continuous femoral and sciatic nerve block. Reg Anesth Pain Med. Sep-Oct 2005;30(5):434-445.
Ilfeld BM, Ball ST, Gearen PF, et al. Health-related quality of life after hip arthroplasty with and without an extended-duration continuous posterior lumbar plexus nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Aug 2009;109(2):586-591.
Ilfeld BM, Meyer RS, Le LT, et al. Health-related quality of life after tricompartment knee arthroplasty with and without an extended-duration continuous femoral nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Apr 2009;108(4):1320-1325.
Feibel RJ, Dervin GF, Kim PR, Beaule PE. Major complications associated with femoral nerve catheters for knee arthroplasty: a word of caution. J Arthroplasty. Sep 2009;24(6 Suppl):132-137.
Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg. Dec 2010;111(6):1552-1554.
Memtsoudis SG, Dy CJ, Ma Y, Chiu YL, Della Valle AG, Mazumdar M. In-hospital patient falls after total joint arthroplasty: incidence, demographics, and risk factors in the United States. J Arthroplasty. Jun 2012;27(6):823-828 e821.
Charous MT, Madison SJ, Suresh PJ, et al. Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block. Anesthesiology. Oct 2011;115(4):774-781.
Ilfeld BM, Moeller LK, Mariano ER, et al. Continuous peripheral nerve blocks: is local anesthetic dose the only factor, or do concentration and volume influence infusion effects as well? Anesthesiology. Feb 2010;112(2):347-354.
Ilfeld BM, Yaksh TL. The end of postoperative pain–a fast-approaching possibility? And, if so, will we be ready? Reg Anesth Pain Med. Mar-Apr 2009;34(2):85-87.
Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand. Jan 2011;55(1):14-19.
Jaeger P, Nielsen ZJ, Henningsen MH, Hilsted KL, Mathiesen O, Dahl JB. Adductor Canal Block versus Femoral Nerve Block and Quadriceps Strength: A Randomized, Double-blind, Placebo-controlled, Crossover Study in Healthy Volunteers. Anesthesiology. Feb 2013;118(2):409-415.
Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. Feb 2012;116(2):248-273.
Perlas A, Kirkham KR, Billing R, et al. The impact of analgesic modality on early ambulation following total knee arthroplasty. Reg Anesth Pain Med. Jul-Aug 2013;38(4):334-339.
Mudumbai SC, Kim TE, Howard SK, et al. Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin Orthop Relat Res. 2014 May;472(5):1377-83.
Originally included in my editorial for the November 2013 issue of ASRA News.
In November 2013 issue of ASRA News, we feature two very special articles that touch on the common theme of global humanitarian aid and volunteerism. Our Resident Section Committee article by Dr. Anish Doshi provides us with an overview of the paucity of pain management and palliative care services in the developing world. As a new column for ASRA News, the Member Spotlight, we present the amazing work of Dr. Randy Malchow and his team in bringing regional anesthesia and perioperative pain management services and education to Kijabe Hospital in Kenya.
I should say that the contents of this editorial/blog are my own opinions and do not necessarily represent the official views of ASRA. The subject of medical volunteerism and global humanitarian aid is important to me, having personally participated in multiple medical missions to underserved communities in the Philippines and Ecuador over the last decade. Many of our ASRA members have dedicated their time and resources to similar causes at home and abroad, and the American Society of Anesthesiologists (ASA) has its own Global Humanitarian Outreach (GHO) Program. The statistics related to anesthesia and pain management in the developing world are quite shocking. It is not uncommon for developing countries to have a ratio of less than 1 anesthesiologist for every 100,000 people! In the realm of pain management and palliative care, the article by Dr. Doshi is particularly eye-opening and should serve as a strong motivator for our members to get involved in helping the underserved. What is the best way to do that?
The GHO offers a search engine for ASA members to look up volunteer opportunities abroad. Not everyone can take weeks or months off work to travel to far-away places. I have been fortunate in that my wife and I have been able to volunteer together—that is, until recently when we started our latest adventure (parenting). In addition, although not naturally a cynic, I find myself questioning the real difference certain medical mission groups make. Even though the before and after photos look great, how much difference does it make to a community when a medical mission group swoops in, repairs some cleft lips, and leaves without every returning? Yes, I understand the social stigma associated with congenital deformities; I have seen it firsthand. However, I also know that there is a bigger picture to consider—patient education on nutrition, prenatal care, and health care maintenance; access to basic resources, including food, shelter, and transportation; and infrastructure improvements that are required to sustain change. Furthermore, does this paternalism actually do damage to future relationships with local health officials and governments within the countries in need, especially when late complications arise after the medical mission groups are long gone?
When you read Dr. Malchow’s article, one of the most impressive features of this program is its sustainability. Not only does this volunteer group provide medical and surgical services to patients in need—a critical part of its “mission” is education of local providers. Under the direction of Dr. Mark Newton, the Vanderbilt International Anesthesia (VIA) program is engaged in an ongoing relationship with Kijabe Hospital; and by training future generations of local anesthesia providers, VIA is raising the quality and safety of anesthesia and pain management services for the entire region. One of the most important messages in Dr. Malchow’s article is that you don’t have to fly to Kenya to make a difference. VIA would not be able to accomplish its goals without the countless people who have donated medical supplies and money for equipment and shipping.
I have been very fortunate to have joined medical mission groups that generally return to the same communities year after year. One of the most rewarding aspects of participating, in my experience, has been developing relationships—with team members, local physicians and nurses, students and residents, government officials, and patients and families. Although we can congratulate ourselves on what we have accomplished so far, there is still so much work left to do.
Imagine — where would elective surgery be today if patients still worried about operating rooms exploding or developing liver and kidney failure from anesthesia?
Having major surgery would be a very different experience without anesthesia. Before the advent of safe anesthesia techniques, the world of surgery was basically limited to amputations and other attempts at life-saving maneuvers. Dr. Bigelow’s publication describing the safe administration of ether changed everything, and the New England Journal of Medicine called this the most important article in its history. With this article, the science and clinical practice of anesthesiology, as well as the modern era of surgery, were born.
How is “anesthesiology” different than “anesthesia?” Anesthesiology is a science like biology or physiology and a field of medicine like cardiology or radiology. Anesthesia, a word with Greek origin, means “without sensation.” There are different types of practitioners who can administer anesthesia, but not all of them are anesthesiologists. The heart of anesthesiology continues to be the patient experience. As anesthesiologists, we are physicians who specialize in relieving anxiety, preventing and treating pain, preventing and managing complications related to surgery, and improving the outcomes for patients who undergo invasive procedures. Not only are we clinicians who apply the best available evidence in our patient care practice; we are the physicians and scientists who develop the evidence. The clinical practice of delivering anesthesia should not take place without the involvement of anesthesiologists.
Often referred to as “going to sleep,” general anesthesia itself is actually not that simple. In fact, there is a lot of science behind the turning of dials that many patients and providers take for granted. Anesthetic agents have not always been as safe as they are today, and anesthesiologists were responsible for conducting important research to retire some of the anesthetics that had the potential to cause patients harm. Thanks to anesthesiologists, we have fast-acting and safe anesthetic gases that have facilitated the evolution of same-day outpatient procedures.
One study that has guided my practice was conducted by my residency advisor, Dr. Alex Macario. His research team surveyed patients having elective surgery to ask them which adverse effects of anesthesia they wish to avoid most. The answers are a little surprising. Two of the top 4 items are nausea and vomiting, with vomiting being #1. To improve the experience for patients undergoing anesthesia, anesthesiologists have studied medications that prevent nausea and vomiting after surgery and have established practice guidelines to share their recommendations with anesthesia providers and patients everywhere.
My own research has focused on developing safe pain management techniques for patients having surgery that decreases the need for narcotics. Like other anesthesiologists before me, I have studied target-specific pain relief techniques using local anesthetic nerve blocks that allow patients to recover at home instead of staying in the hospital for pain control after surgery. What does this mean for you as a patient? It means sleeping better in your own bed in your own house instead of in the hospital. It means using less narcotic pain medication and avoiding the side effects like nausea and constipation that come with it. It means that family members who take care of you at home can do this more easily, and they need to take less time off work. It means that you as a patient can recover more quickly and get back to doing the things you want to do.
I apply my research results and the results of other anesthesiologists’ research studies to my clinical practice every day. I don’t pretend to have all the answers, and I am very wary of those who say they do. Like many of my anesthesiology colleagues, I see potential research questions and opportunities to improve the surgical experience in daily patient care activities, and I am fortunate to work in an environment that supports investigation and inspires innovation.
I have been told that it is difficult sometimes to distinguish an anesthesiologist from other anesthesia providers by what we wear and how we look. That may be true, but there is something special about how anesthesiologists think — how we perceive clinical information, analyze it, interpret it, and apply it — that patients need to know.
Anesthesiologists, working alone or in a care team model supervising other anesthesia providers, bring their expertise to the bedside to improve the patient experience. There has been growing pressure recently to abandon the team model and remove the need for nurse anesthetist supervision. Why are patients and surgeons being forced to choose between having a nurse anesthetist OR an anesthesiologist when they shouldn’t have to? Given the choice, I think they will choose “AND.”
This companion to the recently-released Manual of Clinical Anesthesiology (Chu and Fuller, eds.) focuses on what the clinician needs to know when performing the latest ultrasound-guided regional anesthesia procedures. The format of this book is compact and spiral bound, filled with useful cognitive aids, and each page is laminated to make it fluid-proof (perfect for the operating room).
Anesthesiologists are physicians who promote patient well-being in and out of the operating room. As a diverse group, we can deliver safe anesthesia care in the operating room and procedural areas using a wide array of state-of-the-art technology, provide medical evaluation and consultation for patients before and after surgery, manage pain conditions resulting from surgery or other injuries in the short- and long-term, and discover safer and more effective ways to care for patients in the field of anesthesiology research.
After college, modern anesthesiologists complete four years of medical school then four years of residency training, and many go on to pursue extra years of fellowship training in pediatric or cardiac anesthesiology, acute or chronic pain medicine, critical care medicine, research, or other specialty fields of perioperative care. Anesthesiologists arespecialists in the human condition under stress, mastering the areas of physiology and pharmacology, including the body’s response to potent medications.
Great strides in patient safety have been made by anesthesiologists. Specifically, the use of life-like patient simulation in the training of new physicians was pioneered by anesthesiologists. Research conducted by anesthesiologists at the VA Palo Alto, in part, led to the replacement of toxic (and occasionally explosive) anesthetic gases with the safe agents we use today.It is no exaggeration to say that modern surgery would not exist without the incredible advances in anesthesiology.
I am proud to be an anesthesiologist and follow in the footsteps of giants who have come before me. I have the best job in the world: helping patients through the stressful experience of surgery, relieving pain, and making new discoveries through research that will hopefully benefit future patients.
The application cycle for the 2014-15 Stanford Regional Anesthesiology and Acute Pain Medicine Fellowship class is still open for 1 off-cycle spot scheduled to start in Winter 2015. The application cycle for 2015-16 is also open now and will remain open until Summer 2014. I co-direct this training program along with Dr. Lindsey Vokach-Brodsky. In addition to being the only fellowship in this specialty located in Northern California, the Stanford program provides its fellows with a unique training experience in a beautiful setting.Throughout the training year, various clinical rotations at Stanford Medical Center, Stanford Medicine Outpatient Center, and the VA Palo Alto immerse fellows in an environment focused on teaching them advanced regional anesthesia techniques and perioperative pain medicine.Fellows have ample opportunity to participate in clinical research projects and to teach basic and intermediate techniques to residents and other practitioners at educational workshops and study anatomy in the cadaver lab.
If you are interested in applying, please see the Stanford Anesthesia website for further information. To compare programs, visit ASRA.com.
Edward R. Mariano, MD, MAS, FASA, FASRA is a physician specializing in anesthesiology, professor, husband, and father working to improve pain control, outcomes, and the overall experience for patients having surgery
 Many days I spend in an administrative leadership role or conducting research studies. These functions support the best interests of my patients as well as the science and practice of anesthesiology. On my “clinical” days that I spend in hands-on patient care, I provide anesthesia for patients who undergo surgery and other invasive procedures. I also treat acute pain as a consultant. Some of my colleagues in anesthesiology specialize in chronic pain or critical care medicine.
Many days I spend in an administrative leadership role or conducting research studies. These functions support the best interests of my patients as well as the science and practice of anesthesiology. On my “clinical” days that I spend in hands-on patient care, I provide anesthesia for patients who undergo surgery and other invasive procedures. I also treat acute pain as a consultant. Some of my colleagues in anesthesiology specialize in chronic pain or critical care medicine. re administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.
re administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.






 The application cycle for the 2014-15 Stanford Regional Anesthesiology and Acute Pain Medicine Fellowship class is still open for 1 off-cycle spot scheduled to start in Winter 2015. The application cycle for 2015-16 is also open now and will remain open until Summer 2014.
The application cycle for the 2014-15 Stanford Regional Anesthesiology and Acute Pain Medicine Fellowship class is still open for 1 off-cycle spot scheduled to start in Winter 2015. The application cycle for 2015-16 is also open now and will remain open until Summer 2014.